Pancreatic acinar cell carcinoma is a rare tumor, accounting for only about 1 percent of all pancreatic cancer. The long-term survival for patients with acinar cell carcinoma is significantly better than the long-term survival of patients with pancreatic adenocarcinoma. As no large series of patients with acinar cell carcinomas exist, our understanding of this disease comes mainly from small case series and case reports. Aggressive surgical resection with negative margins is associated with long-term survival in these more favorable pancreatic cancers. There are no clear treatment guidelines for patients in whom complete surgical resection with curative intent is not possible. Acinar cell carcinomas are chemo responsive to agents that have activity against pancreatic adenocarcinomas and colorectal carcinomas because of the shared genetic alterations between these cancers.
Acinar cell carcinomas represent approximately 1–2 percent of adult exocrine pancreatic neoplasms and most occur in late adulthood, with a peak incidence in the 60s. 15 percent of the pediatric exocrine pancreatic neoplasms are acinar cell carcinomas. Pediatric cases account for only 6 percent of acinar cell carcinomas, usually seen in patients of 8–15 years of age, and the entity is uncommon between the ages of 20 and 40 years. Males are affected more frequently than females with a male to female ratio of 3.6:1. There are no known racial associations.
What is Pancreatic Acinar Cell Carcinoma?
Most acinar cell carcinomas are large with an average size of 10 cm and are easily appreciated on radiologic examination. The mass formed by acinar cell carcinomas is often better defined than those formed by ductal adenocarcinomas, which sometimes help in distinguishing the two entities, but the radiologic findings are non-specific. Computerized tomography and magnetic resonance imaging reveal well-defined, large, round to oval masses that enhance homogenously less than the surrounding pancreas or show cystic areas.
Most acinar cell carcinomas present with non-specific symptoms which are related to the mass effect of the neoplasm but sometimes, they may be an incidental finding on microscopic examination. Common non-specific symptoms include weight loss (52 percent), abdominal pain (32 percent), nausea and vomiting (20 percent), melena (12 percent), weakness, anorexia, or diarrhea (8 percent). In contrast to ductal adenocarcinoma, acinar cell carcinoma rarely results in bile duct obstruction and jaundice, which occurs only in 12 percent of patients. Bile duct obstruction is rare in acinar cell carcinoma because they generally push rather than infiltrate into adjacent structures.
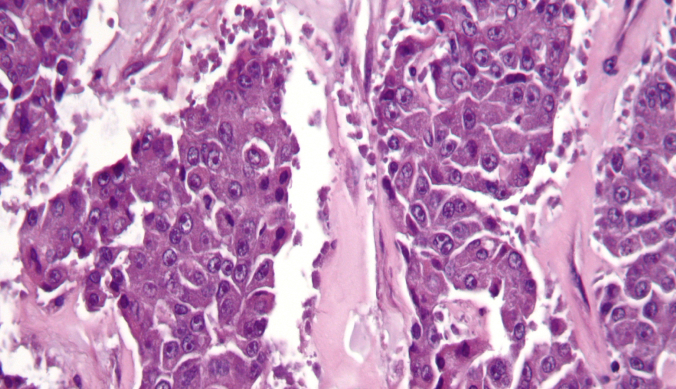
Diagnosis of Acinar Cell Carcinoma
Acinar cell carcinomas are highly aggressive neoplasms, with a median survival for patients with localized disease and metastatic disease of 38 and 14 months, respectively, and an overall 5-year survival rate of less than 10 percent; but this neoplasm is not quite as rapidly lethal as conventional ductal adenocarcinoma. Approximately 50 percent of patients have metastatic disease at the time of diagnosis, and more than half of the remaining patients develop metastatic disease following surgical resection of the primary tumor, but it is not uncommon for patients with distant metastases to survive for 2–3 years. Most often, metastatic disease is found in regional lymph nodes and liver, although occasional patients develop distant metastases to lung, cervical lymph nodes, and ovary. It is rare for patients to present with distant metastases as the first manifestation of the disease. It has been suggested that acinar cell carcinomas occurring under the age of 20 may be less aggressive than their adult counterpart.
The most important prognostic factor is tumor stage, with patients lacking lymph node or distant metastases surviving longer. Patients with the lipase hypersecretion syndrome were shown to have a particularly short survival, because most of these patients had widespread metastatic disease. No specific grading system for acinar cell carcinomas has been proposed. No association between the extent of acinus formation and prognosis has been observed. Other factors that have been correlated with poor outcome include male gender, age over 60, and tumor size greater than 10 cm.
Treatment of Acinar Cell Carcinoma of the Pancreas
Surgical resection is the treatment of choice for patients with early-stage acinar cell carcinoma. Since most of the acinar cell carcinomas are quite large at presentation, they may appear to be unresectable. However, these neoplasms grow in an expansive fashion, rendering even some large carcinomas resectable; so, resection is recommended when feasible. Surgical management is not curative in the majority of patients, but surgical resection seems to be the only available curative treatment of acinar cell carcinomas, the chances of total resection should be surveyed intensively in every case. There is a 72 percent rate of recurrent disease among patients who undergo surgical resection, several of whom experienced distant metastasis as opposed to local recurrences. On multivariate analysis, age less than 65 years, well-differentiated tumors, and negative resection margins are independent prognostic factors for acinar cell carcinoma.
Clinical Trials for Acinar Cell Carcinoma of the Pancreas
Acinar cell carcinoma clinical trials offer access to new, innovative treatments that are not widely available but go through strict, FDA-approved regulatory processes before being approved for use. Clinical trials are one way to get state-of-the-art cancer treatment, and in some cases, they may be the only way to get access to newer treatments. They are also the best way for doctors to learn better methods to treat cancer. Massive Bio guides patients through the most comprehensive clinical trial matching process using our AI-Powered system.
If you have been diagnosed with any of the following pancreatic cancer subtypes, we are here to help:
- Adenocarcinoma (Ductal Carcinoma)
- Acinar Cell Carcinoma
- Squamous Cell Carcinoma
- Adenosquamous Carcinoma
- Colloid Carcinoma
If you do not know which type of pancreatic cancer you have, that is okay. Additional testing can help you determine your exact diagnosis.