Stage Iii Adrenocortical Cancer
Stage III Adrenocortical Cancer is a rare and aggressive malignancy originating in the adrenal cortex, the outer layer of the adrenal glands. This advanced stage indicates that the cancer has spread beyond the adrenal gland, often involving nearby lymph nodes or invading surrounding tissues.

Key Takeaways
- Stage III Adrenocortical Cancer signifies a tumor that has grown beyond the adrenal gland, potentially involving nearby lymph nodes or adjacent organs.
- Symptoms often arise from hormonal overproduction by the tumor or from the physical bulk of the mass pressing on surrounding structures.
- Diagnosis involves imaging, hormone tests, and biopsy to confirm the cancer and its stage.
- Treatment typically includes surgery, often followed by systemic therapies like chemotherapy, to manage the disease.
- The prognosis for Stage III Adrenocortical Cancer is challenging, with outcomes varying based on tumor characteristics and response to treatment.
What is Stage III Adrenocortical Cancer?
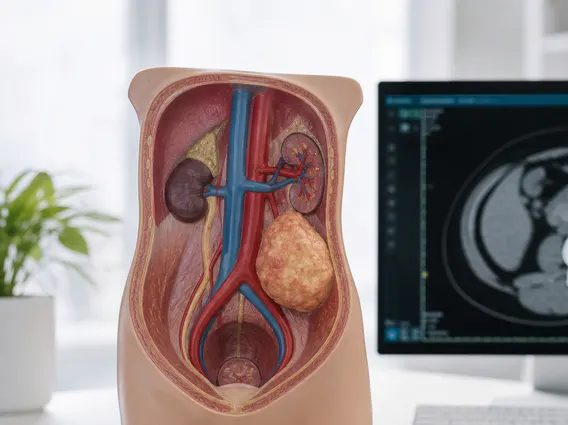
Stage III Adrenocortical Cancer refers to a malignant tumor that has originated in the adrenal cortex and has progressed to a point where it has either invaded surrounding tissues or spread to regional lymph nodes. Adrenocortical carcinoma (ACC) is a rare cancer, with an incidence of about 0.7 to 2 cases per million population per year, as reported by various oncology registries. In Stage III, the tumor may be large and has breached the adrenal capsule, potentially extending into the kidney, diaphragm, or major blood vessels like the vena cava, or it has spread to lymph nodes located near the adrenal gland, but not to distant sites.
Understanding the staging is crucial for determining the appropriate treatment strategy and predicting patient outcomes. This stage represents a more advanced disease state compared to earlier stages, requiring comprehensive and often multidisciplinary management approaches.
Symptoms of Stage III Adrenocortical Carcinoma
The **stage iii adrenocortical carcinoma symptoms** can be varied, often resulting from two main factors: the overproduction of hormones by the cancerous adrenal gland or the physical effects of a large tumor mass. Many ACCs are functional, meaning they secrete excessive amounts of hormones such as cortisol, aldosterone, androgens, or estrogens, leading to distinct clinical syndromes. Non-functional tumors primarily cause symptoms due to their size and pressure on adjacent organs.
Common symptoms associated with Stage III Adrenocortical Carcinoma include:
- Hormonal Imbalance:
- Cushing’s syndrome (due to excess cortisol): weight gain, muscle weakness, high blood pressure, diabetes, easy bruising, and facial rounding.
- Virilization (due to excess androgens, more common in females): hirsutism (excess body hair), deepening voice, male-pattern baldness, and menstrual irregularities.
- Feminization (due to excess estrogens, more common in males): breast enlargement (gynecomastia), decreased libido, and testicular atrophy.
- Conn’s syndrome (due to excess aldosterone): high blood pressure and low potassium levels.
- Mass Effect:
- Abdominal pain or discomfort, often vague and persistent.
- A palpable mass in the abdomen.
- Feeling of fullness or bloating.
- Back pain, if the tumor is pressing on nerves or invading surrounding structures.
- Weight loss and fatigue, which are general signs of advanced cancer.
Due to the rarity of the disease and the non-specific nature of many symptoms, diagnosis can sometimes be delayed until the cancer has reached a more advanced stage.
Treatment and Prognosis for Stage III Adrenocortical Cancer
The **treatment for stage 3 adrenocortical cancer** is complex and typically involves a multidisciplinary approach due to the advanced nature of the disease. The primary treatment modality, whenever feasible, is surgical resection. Complete surgical removal of the tumor and any involved regional lymph nodes offers the best chance for long-term survival. However, achieving complete resection can be challenging in Stage III due to tumor size and local invasion.
Following surgery, or if surgery is not possible, systemic therapies are often employed. These may include:
- Adjuvant Therapy: Mitotane, an adrenolytic agent, is frequently used after surgery to reduce the risk of recurrence.
- Chemotherapy: Regimens often involve drugs like etoposide, doxorubicin, cisplatin, and mitotane (EDP-M) to target cancer cells throughout the body.
- Radiation Therapy: May be used to control local symptoms or to treat areas where the tumor could not be completely removed.
- Targeted Therapy: In some cases, based on molecular profiling of the tumor, targeted therapies that block specific pathways involved in cancer growth may be considered.
The **prognosis of stage iii adrenocortical cancer** is generally less favorable compared to earlier stages, reflecting the extent of disease spread. Survival rates vary significantly depending on several factors, including the completeness of surgical resection, the tumor’s biological aggressiveness, and the patient’s response to systemic therapies. According to data from the National Cancer Institute’s SEER program, the 5-year relative survival rate for localized adrenocortical carcinoma is higher than for regional disease (which includes Stage III). While specific statistics for Stage III can vary, medical experts generally indicate a more guarded prognosis, emphasizing the importance of aggressive and tailored treatment plans.
Ongoing research continues to explore new therapeutic strategies and improve outcomes for patients with this challenging cancer.