Burkitt Leukemia
Burkitt leukemia is a highly aggressive form of B-cell non-Hodgkin lymphoma, characterized by rapid growth and spread. It is considered an oncologic emergency due to its fast progression and potential for severe complications.

Key Takeaways
- Burkitt leukemia is an aggressive B-cell lymphoma that often presents as leukemia, characterized by rapid cell growth.
- It is strongly associated with certain risk factors, including Epstein-Barr virus (EBV) infection, particularly in endemic regions.
- Symptoms can develop quickly and include swollen lymph nodes, abdominal swelling, and neurological issues.
- Diagnosis involves biopsy and genetic testing, while treatment typically involves intensive chemotherapy regimens.
- Early diagnosis and aggressive treatment are crucial for improving outcomes due to its rapid progression.
What is Burkitt Leukemia? Definition, Types, and Symptoms
Burkitt leukemia refers to a rare and highly aggressive type of B-cell non-Hodgkin lymphoma where the cancerous cells are found in the bone marrow and peripheral blood, resembling acute leukemia. This condition is characterized by the rapid proliferation of immature B-lymphocytes, leading to a swift onset of symptoms. It is named after Denis Burkitt, who first described the disease in African children in 1958. The defining characteristic is a chromosomal translocation involving the MYC gene, which drives uncontrolled cell growth.
There are three main clinical variants of Burkitt leukemia, though all share similar pathological features: endemic, sporadic, and immunodeficiency-associated. Endemic Burkitt leukemia is prevalent in equatorial Africa and is strongly linked to Epstein-Barr virus (EBV) infection and malaria. Sporadic Burkitt leukemia occurs worldwide and is less frequently associated with EBV. Immunodeficiency-associated Burkitt leukemia is seen in individuals with compromised immune systems, such as those with HIV/AIDS or organ transplant recipients.
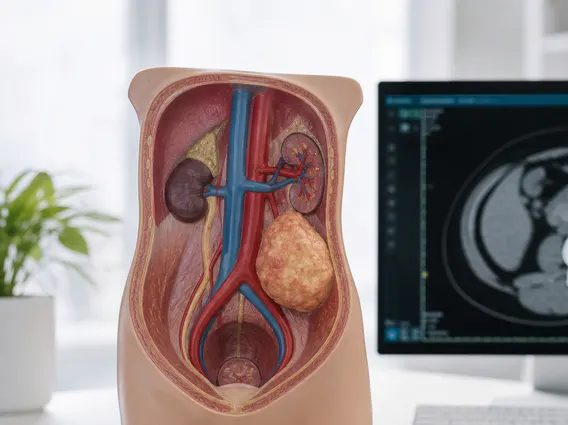
The **Burkitt leukemia definition and symptoms** often include rapidly enlarging lymph nodes, particularly in the neck, armpits, or groin. Other common symptoms can manifest quickly due to the rapid proliferation of cancer cells:
- Abdominal swelling and pain, often due to tumor involvement in the intestines or ovaries.
- Jaw or facial swelling, especially in endemic forms.
- Fatigue and weakness.
- Fever and night sweats.
- Unexplained weight loss.
- Neurological symptoms if the central nervous system is involved, such as headaches, vision changes, or paralysis.
While closely related, it is important to distinguish between Burkitt lymphoma and Burkitt leukemia. The distinction primarily lies in the extent of bone marrow involvement and the presence of circulating cancer cells in the blood. The table below highlights key differences:
| Feature | Burkitt Lymphoma | Burkitt Leukemia |
|---|---|---|
| Primary Presentation | Solid tumor masses (e.g., abdomen, jaw, lymph nodes) | High percentage of blast cells in bone marrow and peripheral blood |
| Bone Marrow Involvement | Typically less than 25% blast cells | Greater than 25% blast cells, often much higher |
| Circulating Cells | Few or no circulating lymphoma cells | Numerous circulating lymphoma cells (leukemic phase) |
| Diagnostic Criteria | Primarily tissue biopsy of solid tumor | Bone marrow biopsy and peripheral blood analysis |
This distinction, particularly the **Burkitt lymphoma vs leukemia** presentation, guides diagnostic approaches and treatment strategies, though both are aggressive B-cell malignancies.
Causes and Risk Factors for Burkitt Leukemia
The development of Burkitt leukemia is primarily driven by a characteristic genetic abnormality: a chromosomal translocation involving the MYC oncogene. This translocation typically moves the MYC gene from chromosome 8 to chromosome 14, 2, or 22, placing it under the control of highly active immunoglobulin gene enhancers. This leads to the overexpression of the MYC protein, which promotes uncontrolled cell growth and division.
Beyond this genetic hallmark, several environmental and infectious factors contribute to the **causes and risk factors for Burkitt leukemia**. In endemic regions, Epstein-Barr virus (EBV) infection is a significant risk factor, found in nearly all cases. EBV is thought to play a role in promoting B-cell proliferation and hindering immune surveillance, creating an environment conducive to MYC translocation. Chronic malaria infection is also a co-factor in endemic areas, as it can lead to chronic B-cell stimulation and immunosuppression, further increasing susceptibility to EBV-driven lymphomagenesis. According to the World Health Organization (WHO), EBV is associated with approximately 1-2% of all cancers globally, with Burkitt leukemia being one of the most notable.
For sporadic and immunodeficiency-associated forms, while EBV may still be present, other factors are more prominent. Immunodeficiency, particularly in individuals with HIV/AIDS, significantly increases the risk. The weakened immune system in these patients is less effective at controlling viral infections and eliminating abnormal B-cells, making them more vulnerable to developing aggressive lymphomas like Burkitt leukemia.
Diagnosing and Treating Burkitt Leukemia
Accurate **Burkitt leukemia diagnosis and treatment** are critical due to the disease’s aggressive nature. Diagnosis typically begins with a thorough physical examination and blood tests, which may reveal a high white blood cell count with characteristic blast cells. A bone marrow biopsy is essential to confirm the presence of more than 25% blast cells, which is a key diagnostic criterion for the leukemic presentation. Lymph node or tumor biopsies are also performed to examine the cellular morphology and immunophenotype, confirming the B-cell origin and characteristic “starry sky” pattern under microscopy.
Further diagnostic tests include cytogenetic analysis to detect the MYC gene translocation, which is pathognomonic for Burkitt leukemia. Lumbar puncture (spinal tap) is often performed to check for central nervous system involvement, as this can influence treatment decisions. Imaging studies like CT scans, PET scans, and MRI scans help determine the extent of disease spread throughout the body.
Given its rapid progression, **treatment** for Burkitt leukemia is intensive and typically involves multi-agent chemotherapy regimens. These protocols are designed to be highly aggressive to quickly eliminate the fast-growing cancer cells. Common chemotherapy drugs include cyclophosphamide, vincristine, doxorubicin, and methotrexate, often administered in combination. Due to the high risk of central nervous system involvement, intrathecal chemotherapy (medication delivered directly into the spinal fluid) is a standard component of treatment. In some cases, targeted therapies or immunotherapy may be used, particularly in relapsed or refractory disease. The prognosis for Burkitt leukemia has significantly improved with modern intensive chemotherapy, with cure rates reaching 70-90% in children and 50-70% in adults, though early diagnosis remains paramount for optimal outcomes.