High Grade Ductal Carcinoma In Situ
High Grade Ductal Carcinoma In Situ (DCIS) is a non-invasive form of breast cancer where abnormal cells are found in the milk ducts but have not spread to surrounding breast tissue. Understanding this condition is crucial for early detection and effective management.
Key Takeaways
- High Grade Ductal Carcinoma In Situ is a non-invasive breast condition where abnormal cells are confined to the milk ducts.
- It is often asymptomatic and typically detected through routine mammograms.
- Diagnosis involves imaging, biopsy, and pathological examination to determine grade and characteristics.
- Treatment options range from surgery (lumpectomy or mastectomy) to radiation therapy, sometimes with endocrine therapy.
- The prognosis for High Grade DCIS is generally excellent, especially with appropriate treatment.
What is High Grade Ductal Carcinoma In Situ (DCIS)?
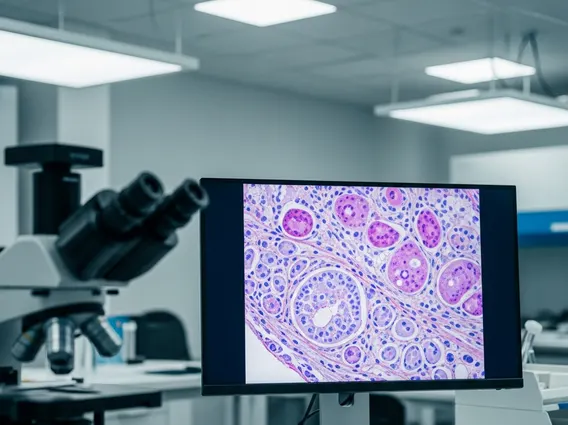
High Grade Ductal Carcinoma In Situ (DCIS) is a non-invasive breast condition characterized by the presence of abnormal cells within the milk ducts of the breast. These cells have not broken through the duct walls to invade the surrounding breast tissue or spread to other parts of the body. The “high grade” designation refers to the aggressive appearance of these cells under a microscope, indicating a higher potential for them to become invasive if left untreated compared to low or intermediate-grade DCIS. While not invasive cancer itself, it is considered a precursor to invasive breast cancer.
DCIS is classified into different grades based on how abnormal the cells look and how quickly they are dividing. High-grade DCIS cells grow and divide more rapidly and have a greater tendency to spread outside the ducts over time if not treated. According to the American Cancer Society, DCIS accounts for about 20% of all newly diagnosed breast cancers in the United States, with a significant portion being high grade.
High Grade DCIS: Symptoms and Diagnosis
High grade DCIS symptoms and diagnosis typically involve the absence of noticeable symptoms, as the condition rarely causes a palpable lump or pain. It is most frequently discovered during routine screening mammograms, which can detect microcalcifications—tiny calcium deposits within the breast tissue that are often associated with DCIS. In some rare cases, a woman might notice a lump or nipple discharge, but these are less common indicators of DCIS.
The diagnostic process usually begins with an abnormal mammogram finding. Further imaging, such as diagnostic mammography or ultrasound, may be performed to get a clearer view of the suspicious area. If imaging suggests DCIS, a biopsy is necessary to confirm the diagnosis. This involves taking a small tissue sample from the suspicious area, often guided by imaging (stereotactic biopsy or ultrasound-guided biopsy), which is then examined by a pathologist. The pathologist determines the grade of the DCIS (low, intermediate, or high) and checks for other characteristics, such as the presence of comedonecrosis (dead cells in the center of the ducts), which is often associated with high-grade DCIS.
Treatment Options and Prognosis for High Grade DCIS
Treatment options for high grade DCIS are primarily aimed at removing the abnormal cells and reducing the risk of developing invasive breast cancer in the future. The main treatment modalities include surgery, often followed by radiation therapy, and sometimes endocrine therapy.
Surgical options typically involve:
- Lumpectomy (breast-conserving surgery): This procedure removes the DCIS and a small margin of healthy tissue around it, preserving most of the breast. It is often followed by radiation therapy to the remaining breast tissue to reduce the risk of recurrence.
- Mastectomy: In some cases, especially for large areas of DCIS, multiple areas of DCIS, or if a lumpectomy cannot achieve clear margins, a total mastectomy (removal of the entire breast) may be recommended. Radiation therapy is usually not needed after a mastectomy for DCIS.
For hormone receptor-positive DCIS, endocrine therapy (such as tamoxifen or aromatase inhibitors) may be prescribed for several years after surgery to further reduce the risk of recurrence in either breast. This decision is made based on individual patient factors and the characteristics of the DCIS.
The prognosis of high grade ductal carcinoma in situ is generally excellent, with very high survival rates. When properly treated, the vast majority of individuals with DCIS do not go on to develop invasive breast cancer or die from the disease. The 5-year survival rate for women diagnosed with DCIS is nearly 100%, according to the National Cancer Institute’s SEER program data. However, there is a small risk of recurrence, either as DCIS or as invasive cancer, in the treated breast or the opposite breast. Regular follow-up appointments and continued screening mammograms are crucial for monitoring and early detection of any potential recurrence.