Isolated Hepatic Perfusion
Isolated Hepatic Perfusion is a highly specialized regional chemotherapy technique designed to deliver high doses of anti-cancer drugs directly to the liver while minimizing systemic exposure. This advanced medical procedure offers a targeted approach for treating certain liver malignancies.

Key Takeaways
- Isolated Hepatic Perfusion (IHP) is a regional chemotherapy treatment for liver cancers.
- It involves surgically isolating the liver’s blood supply to deliver concentrated chemotherapy drugs.
- The procedure aims to maximize drug exposure to liver tumors while reducing side effects on the rest of the body.
- IHP is primarily used for unresectable primary or metastatic liver cancers, particularly those resistant to systemic chemotherapy.
- Patient selection is crucial, involving a multidisciplinary team to assess suitability and potential benefits.
What is Isolated Hepatic Perfusion?
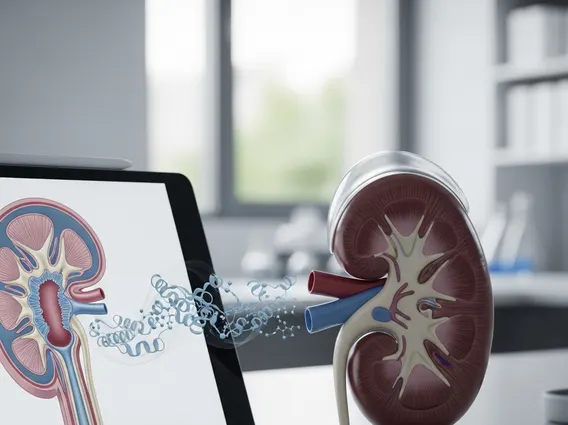
Isolated Hepatic Perfusion (IHP) refers to a complex surgical procedure that allows for the delivery of high-dose chemotherapy directly to the liver, bypassing the rest of the body’s circulation. This technique is employed to treat liver tumors that are either primary (originating in the liver) or metastatic (spread to the liver from another part of the body). The core principle behind IHP is to isolate the liver’s blood supply temporarily, enabling oncologists to administer chemotherapy agents at concentrations significantly higher than what would be tolerated systemically, thereby enhancing their anti-tumor effect while minimizing severe systemic side effects. The process involves cannulating the hepatic artery and portal vein to establish an extracorporeal circuit, which allows blood to be shunted away from the liver, perfused with chemotherapy, and then filtered before being returned to the patient’s general circulation. This targeted delivery mechanism is crucial for managing advanced liver cancers.
The Isolated Hepatic Perfusion Procedure
The isolated hepatic perfusion procedure is a meticulous surgical undertaking requiring a highly skilled multidisciplinary team. It typically begins with a laparotomy to expose the liver and its surrounding vasculature. The key steps involved are:
- Vascular Isolation: The blood vessels supplying and draining the liver (hepatic artery, portal vein, and hepatic veins) are carefully identified and temporarily clamped. This creates a closed circuit for the liver, separating it from the systemic circulation.
- Cannulation: Catheters are then inserted into the hepatic artery and portal vein to deliver the chemotherapy, and into the hepatic veins to collect the outflow.
- Extracorporeal Circuit Connection: The liver is connected to an extracorporeal perfusion circuit, similar to a heart-lung machine. This circuit includes a pump, an oxygenator, and a heat exchanger to maintain physiological conditions.
- Chemotherapy Delivery: High-dose chemotherapy drugs, often melphalan, are infused directly into the isolated liver via the perfusion circuit for a specific duration, typically 60-90 minutes.
- Drug Washout and Reperfusion: After the perfusion period, the chemotherapy agents are thoroughly washed out from the liver using a special solution. The blood is then filtered to remove residual drug before the clamps are removed, and normal blood flow to the liver is restored.
Throughout the procedure, vital signs and drug levels are closely monitored to ensure patient safety and optimize treatment efficacy.
Isolated Hepatic Perfusion for Liver Cancer
Isolated Hepatic Perfusion for liver cancer represents a vital treatment option, particularly for patients with unresectable tumors or those who have not responded to conventional systemic chemotherapy. This includes primary liver cancers like hepatocellular carcinoma (HCC) in select cases, and more commonly, metastatic cancers such as ocular melanoma, neuroendocrine tumors, and colorectal cancer that have spread to the liver. The rationale for using IHP in these scenarios is to concentrate the anti-cancer effect directly on the liver tumors, which are often the primary site of disease progression and mortality. By delivering a high dose of chemotherapy locally, IHP aims to achieve significant tumor reduction or even complete remission, improving patient outcomes and quality of life. According to a study published in the Journal of Clinical Oncology, IHP has shown promising response rates, with some studies reporting objective response rates exceeding 50% for certain types of liver metastases, such as those from ocular melanoma. Patient selection for IHP is critical, involving a comprehensive evaluation by a multidisciplinary team, including surgical oncologists, medical oncologists, and interventional radiologists, to determine suitability and potential benefits versus risks.