
Infiltrating Lobular Carcinoma
Infiltrating Lobular Carcinoma is a distinct type of breast cancer that originates in the milk-producing glands (lobules) of the breast and spreads into surrounding breast tissue. Understanding this condition is crucial for effective diagnosis and treatment.
Key Takeaways
- Infiltrating Lobular Carcinoma (ILC) is the second most common type of invasive breast cancer, accounting for 10-15% of cases.
- ILC cells typically grow in a single-file pattern, making it challenging to detect through standard imaging like mammograms.
- Symptoms can be subtle, often presenting as a thickening or fullness in the breast rather than a distinct lump.
- Diagnosis frequently requires a combination of imaging, physical exam, and biopsy to confirm.
- Treatment strategies for ILC are often multi-modal, including surgery, radiation, chemotherapy, and hormone therapy.
What is Infiltrating Lobular Carcinoma?
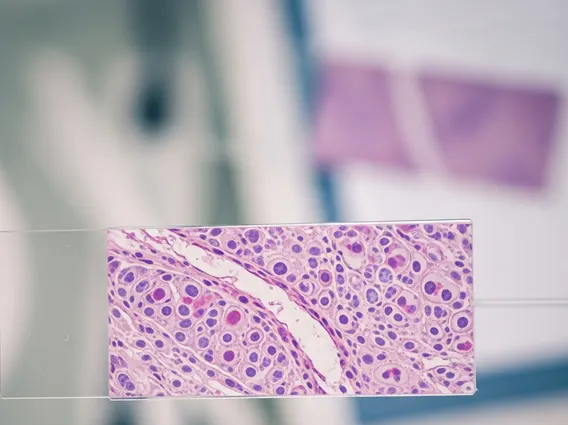
Infiltrating Lobular Carcinoma (ILC) is a form of invasive breast cancer that begins in the milk-producing glands, known as lobules, and then spreads beyond them into the surrounding breast tissue and potentially to other parts of the body. Unlike ductal carcinoma, which originates in the milk ducts, ILC cells tend to grow in a single-file pattern, making them difficult to detect as a distinct mass on physical examination or standard imaging tests. This diffuse growth pattern is a hallmark characteristic that distinguishes it from other breast cancer types.
This type of cancer accounts for approximately 10% to 15% of all invasive breast cancers, making it the second most common form after invasive ductal carcinoma. According to the American Cancer Society, ILC is more often hormone receptor-positive, meaning its growth is fueled by estrogen and/or progesterone. This characteristic significantly influences the choice of treatment options, particularly the use of hormone-blocking therapies. Its unique growth pattern can also lead to it being larger at diagnosis compared to other breast cancers, as it can spread without forming a palpable lump.
Identifying Infiltrating Lobular Carcinoma: Symptoms and Diagnosis
Recognizing infiltrating lobular carcinoma symptoms can be challenging due to its diffuse growth pattern. Unlike the firm, distinct lump often associated with other breast cancers, ILC may present more subtly. Common symptoms can include a thickening or fullness in a specific area of the breast, a change in the breast’s texture or size, or a flattened or inverted nipple. Some individuals might notice a persistent area of swelling or a dimpling of the skin. Because these signs can be indistinct, they are sometimes overlooked or mistaken for normal breast changes.
The infiltrating lobular carcinoma diagnosis often requires a comprehensive approach. A physical examination by a healthcare provider is the first step, followed by imaging tests. While mammograms are standard, ILC’s diffuse nature can make it harder to spot on these scans. Therefore, additional imaging such as ultrasound or magnetic resonance imaging (MRI) is frequently used to better visualize the extent of the cancer. The definitive diagnosis is made through a biopsy, where a small tissue sample is removed from the suspicious area and examined under a microscope by a pathologist. This allows for confirmation of ILC and assessment of its specific characteristics, such as hormone receptor status.
Treatment Options for Infiltrating Lobular Carcinoma
The treatment for infiltrating lobular carcinoma is typically multi-modal, tailored to the individual patient based on the cancer’s stage, size, hormone receptor status, and other factors. Surgical intervention is almost always the primary treatment. This may involve a lumpectomy, which removes only the cancerous tissue and a margin of healthy tissue, or a mastectomy, which removes the entire breast. Due to ILC’s tendency for multi-centricity (occurring in more than one area of the breast) and its diffuse growth, a mastectomy might be recommended more often than for other breast cancer types.
Following surgery, additional therapies are often employed to reduce the risk of recurrence. Radiation therapy may be used after a lumpectomy to destroy any remaining cancer cells in the breast. Chemotherapy is considered for cases where the cancer has spread to lymph nodes or if there are other high-risk features. Given that ILC is frequently hormone receptor-positive, hormone therapy, such as tamoxifen or aromatase inhibitors, is a cornerstone of treatment. These medications work by blocking the effects of estrogen, thereby inhibiting cancer cell growth. Targeted therapies may also be an option depending on specific molecular characteristics of the tumor, offering a personalized approach to care.



















