Malignant Peripheral Nerve Sheath Tumor
Malignant Peripheral Nerve Sheath Tumor (MPNST) is a rare and aggressive type of cancer that originates from the cells surrounding peripheral nerves. Understanding this complex condition is crucial for effective management and improved patient outcomes.

Key Takeaways
- MPNST is a rare, highly aggressive soft tissue sarcoma.
- Approximately half of MPNST cases are associated with Neurofibromatosis Type 1 (NF1).
- Common symptoms include a rapidly growing mass, persistent pain, and neurological deficits.
- Diagnosis relies on imaging studies, followed by a definitive biopsy.
- Treatment primarily involves surgical removal, often supplemented with radiation therapy and chemotherapy.
What is Malignant Peripheral Nerve Sheath Tumor?
Malignant Peripheral Nerve Sheath Tumor (MPNST) is a rare and highly aggressive form of soft tissue sarcoma that arises from the Schwann cells or fibroblasts that form the protective sheath around peripheral nerves. These tumors can develop anywhere in the body where peripheral nerves are present, but they are most commonly found in the extremities, trunk, and head and neck regions. MPNST is a particularly challenging cancer due to its aggressive nature and tendency to recur and metastasize.
MPNST accounts for approximately 5-10% of all soft tissue sarcomas. A significant proportion, about 50%, of MPNSTs occur in individuals with Neurofibromatosis Type 1 (NF1), a genetic disorder that predisposes individuals to nerve sheath tumors. In these cases, MPNST often develops from pre-existing benign plexiform neurofibromas. For individuals without NF1, MPNST can arise spontaneously or sometimes after radiation exposure.
Malignant Peripheral Nerve Sheath Tumor Symptoms and Diagnosis
Recognizing malignant peripheral nerve sheath tumor symptoms is critical for early intervention, though they can be non-specific initially. Symptoms typically include a rapidly growing mass, often accompanied by pain that may be constant, worsening, or radiating along the nerve. Neurological deficits such as weakness, numbness, tingling, or loss of function in the affected limb or area may also occur as the tumor compresses or invades the nerve.
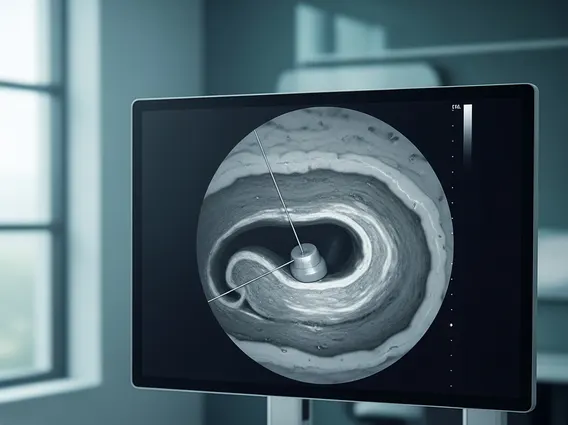
The diagnosis of malignant peripheral nerve sheath tumor involves a comprehensive approach. It usually begins with a thorough physical examination and a detailed medical history. Imaging studies are crucial for localizing the tumor, assessing its size, and determining its relationship to surrounding structures. Magnetic Resonance Imaging (MRI) is often the preferred modality for its excellent soft tissue contrast, while Computed Tomography (CT) scans may be used to evaluate bone involvement or distant metastases. Positron Emission Tomography (PET) scans can help assess metabolic activity and identify potential spread. The definitive diagnosis, however, is established through a biopsy (either incisional or excisional), where tissue samples are taken and examined by a pathologist for characteristic features of MPNST.
Common symptoms that may prompt investigation include:
- A palpable lump or mass that is rapidly increasing in size.
- Persistent or worsening pain that is not relieved by typical pain medication.
- New or worsening neurological symptoms, such as muscle weakness or numbness.
- Changes in skin sensation or motor function in an area supplied by a peripheral nerve.
Malignant Peripheral Nerve Sheath Tumor Treatment
The primary approach to malignant peripheral nerve sheath tumor treatment is aggressive surgical resection. The goal of surgery is to achieve a complete removal of the tumor with clear margins, meaning no cancer cells are left behind at the edges of the removed tissue. This is often challenging due to the tumor’s infiltrative nature and its close proximity to vital nerves and blood vessels. In some cases, limb amputation may be necessary to achieve clear margins, particularly for tumors in the extremities.
Adjuvant therapies, such as radiation therapy, are frequently used in conjunction with surgery to improve local control and reduce the risk of recurrence. Radiation therapy may be administered before surgery (neoadjuvant) to shrink the tumor and make it easier to remove, or after surgery (adjuvant) to eliminate any remaining microscopic cancer cells. Chemotherapy may also be considered, particularly for high-grade tumors, large tumors, or those that have metastasized, although its effectiveness in MPNST is still an area of ongoing research and can vary among patients.