Prcc
Prcc, or Papillary Renal Cell Carcinoma, is a distinct subtype of kidney cancer that originates in the lining of the small tubes in the kidney. Understanding this condition is crucial for accurate diagnosis and effective treatment strategies.

Key Takeaways
- Prcc (Papillary Renal Cell Carcinoma) is the second most common type of kidney cancer, accounting for 10-15% of all renal cell carcinomas.
- It is characterized by distinct histological patterns, typically categorized into Type 1 and Type 2, with varying genetic associations and prognoses.
- Diagnosis often involves imaging studies and sometimes biopsy, while management primarily relies on surgical removal of the tumor.
- Targeted therapies and immunotherapies are emerging treatment options for advanced or metastatic Prcc.
- Early detection and a comprehensive understanding of its specific characteristics are vital for optimizing patient outcomes.
What is Prcc?
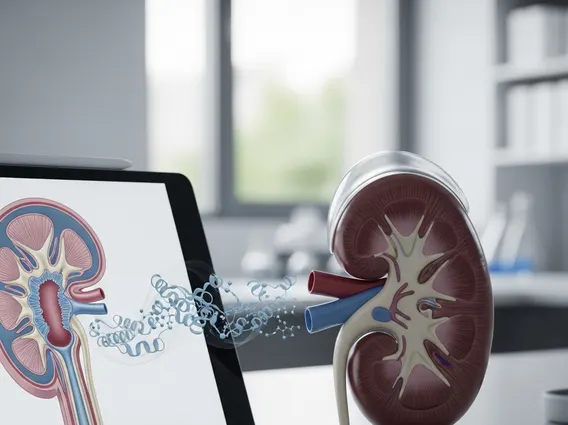
Prcc meaning refers to Papillary Renal Cell Carcinoma, a specific type of kidney cancer. This condition is characterized by the growth of finger-like projections (papillae) within the tumor cells, which distinguishes it from other forms of renal cell carcinoma. The Prcc definition describes it as a malignant tumor arising from the renal tubular epithelium, representing the second most common subtype of kidney cancer after clear cell renal cell carcinoma.
For those seeking to have Prcc explained, it is important to note that it accounts for approximately 10-15% of all renal cell carcinomas. While generally considered less aggressive than clear cell RCC, its clinical behavior can vary significantly, particularly between its two main subtypes. Understanding these distinctions is fundamental for appropriate patient care and research.
Characteristics and Clinical Significance of Prcc
Papillary Renal Cell Carcinoma (Prcc) is histologically divided into two main types, each with unique characteristics and clinical implications. Type 1 Prcc typically presents as smaller tumors, often multifocal, and is associated with mutations in the MET proto-oncogene. These tumors are generally less aggressive and have a more favorable prognosis.
Type 2 Prcc, on the other hand, tends to be more aggressive, often larger, and can be associated with various genetic alterations, including those in the fumarate hydratase (FH) gene in some hereditary forms. The distinction between these types is crucial for prognosis and treatment planning. According to the American Cancer Society, kidney cancer, including Prcc, is more common in men and typically diagnosed in older adults, with an average age of diagnosis around 64.
The clinical significance of Prcc lies in its diverse presentation and varying prognoses. While many cases are indolent, particularly Type 1, some Type 2 tumors can be highly aggressive, necessitating different therapeutic approaches. Understanding these characteristics helps clinicians tailor treatment strategies and predict patient outcomes more accurately.
Diagnosis and Management of Prcc
The diagnosis of Prcc typically begins with imaging studies such as ultrasound, computed tomography (CT) scans, or magnetic resonance imaging (MRI) when a kidney mass is suspected. These imaging modalities can help characterize the tumor, assess its size, location, and potential spread. While imaging can suggest the presence of Prcc, a definitive diagnosis often requires a tissue biopsy, though this can be challenging due to the tumor’s location and the risk of complications.
Management of Prcc largely depends on the stage and type of the cancer. For localized tumors, surgical resection is the primary treatment. This may involve a partial nephrectomy (removing only the tumor and a margin of healthy tissue) or a radical nephrectomy (removing the entire kidney), depending on the tumor’s size and location. For advanced or metastatic Prcc, systemic therapies are employed. These include:
- Targeted Therapies: Medications that specifically block pathways involved in cancer growth, such as VEGF inhibitors (e.g., sunitinib, pazopanib) or MET inhibitors (e.g., cabozantinib, savolitinib), particularly relevant for Type 1 Prcc.
- Immunotherapy: Treatments that harness the body’s immune system to fight cancer, such as checkpoint inhibitors (e.g., nivolumab, pembrolizumab).
- Clinical Trials: Participation in clinical trials offers access to novel therapies for patients with advanced disease.
Post-treatment surveillance is essential to monitor for recurrence or progression. This typically involves regular imaging and blood tests. While alternative or complementary therapies may be discussed, it is crucial to understand that such information is supportive only and does not replace conventional medical treatment for Prcc.