Pedunculated
In medicine, the term ‘pedunculated’ describes a specific morphological characteristic of lesions, growths, or tumors. Understanding this term is crucial for accurate diagnosis and treatment planning in various clinical settings.
Key Takeaways
- Pedunculated lesions are attached to a broader surface by a narrow stalk or pedicle.
- This morphology is common in polyps, fibroids, and certain skin lesions.
- The presence of a stalk can influence diagnostic imaging and surgical removal techniques.
- It contrasts with sessile lesions, which have a broad, flat base directly attached to the surface.
What is Pedunculated: Medical Definition and Characteristics
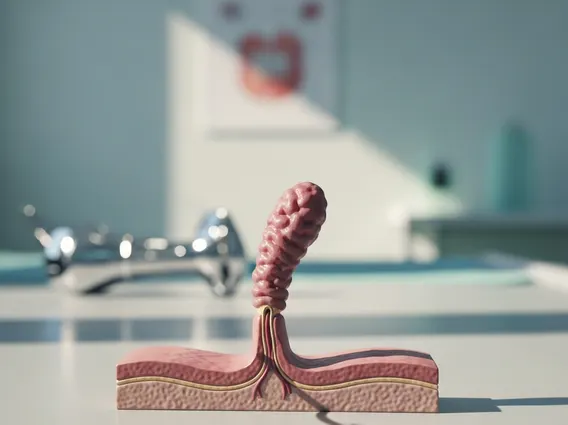
The term pedunculated meaning medical describes a growth, lesion, or tumor that is attached to a broader surface by a narrow, stalk-like structure known as a pedicle. This distinct morphological feature means the main body of the lesion is elevated away from the underlying tissue, connected solely by this slender stem. The pedunculated lesion definition specifically emphasizes this unique attachment, which serves as a key differentiator from other types of growths.
Key characteristics of pedunculated lesions include:
- A distinct stalk or pedicle: This connecting stem is always narrower than the main body of the lesion, though its length and thickness can vary significantly.
- Elevated position: The lesion’s main mass sits above the surrounding tissue, supported by its stalk.
- Potential for mobility: Depending on the length and flexibility of the pedicle, pedunculated lesions may exhibit some degree of movement, which can be observed during physical examination or diagnostic imaging.
- Diverse locations: These lesions can manifest in various anatomical sites, such as the gastrointestinal tract (e.g., colorectal polyps), the uterus (e.g., certain uterine fibroids), on the skin (e.g., skin tags), or within the vocal cords.
The presence of a pedicle holds significant clinical implications. For instance, a long or thin stalk can sometimes twist (torsion), potentially compromising the blood supply to the lesion and leading to complications such as ischemia or necrosis. Furthermore, the stalk provides a natural point for surgical removal, often allowing for less invasive procedures like snare polypectomy in the colon. Understanding these characteristics is vital for accurate diagnosis and effective management.
Pedunculated vs. Sessile: Understanding the Difference
The distinction between pedunculated vs sessile lesions is a fundamental concept in medical terminology, primarily concerning their mode of attachment to the underlying tissue. While pedunculated lesions are characterized by their narrow stalk, sessile lesions are defined by a broad, flat base that attaches directly to the surface without an intervening pedicle. This morphological difference carries significant clinical implications, influencing how these lesions are identified, biopsied, and ultimately removed. For example, sessile lesions, due to their wide attachment, can sometimes be more challenging to completely excise, potentially requiring more extensive surgical margins or specialized endoscopic techniques to ensure full removal and reduce recurrence risk.
| Feature | Pedunculated Lesion | Sessile Lesion |
|---|---|---|
| Attachment | Attached by a narrow stalk (pedicle) | Attached by a broad, flat base |
| Shape | Mushroom-like or cauliflower-like, elevated from surface | Flat, dome-shaped, or mound-like, directly on surface |
| Mobility | Often mobile due to the stalk, allowing for some movement | Generally fixed or less mobile, firmly attached |
| Removal Considerations | Typically easier to remove with a snare or shave excision targeting the stalk, often less invasive | May require wider or more complex excision due to broad base; higher risk of incomplete removal if not carefully managed |
| Clinical Significance | Stalk can twist (torsion); often easier to distinguish from surrounding tissue | Can be harder to detect and delineate; may have a higher risk of harboring invasive cancer, especially if large |
| Common Examples | Many colon polyps, skin tags, some uterine fibroids, certain vocal cord polyps | Some colon polyps (e.g., flat adenomas), certain skin lesions, early cancers, some gastric polyps |
The prevalence of growths that can exhibit either morphology is considerable. Colorectal polyps, for instance, are a common finding, affecting a significant portion of the adult population. The Centers for Disease Control and Prevention (CDC) indicates that regular screening is crucial, as polyps, whether pedunculated or sessile, can potentially develop into cancer. The specific morphology of a polyp is a critical factor in assessing its malignant potential and guiding the most appropriate management strategy, from surveillance to endoscopic or surgical removal.